

Introduction
Understanding factors that influence participant retention is critical for the success of longitudinal research. Failures in retention can reduce promising scientific discovery to unusable data if the sample becomes biased or reduced in size or variability and thus no longer sufficient for the intended analyses. The process of retention begins at recruitment. Participants’ understanding of study goals and potential burden help facilitate informed decision-making for enrollment and commitment to remain in the study (Ely and Coleman 2007; Hunt and White 1998). While some correlates of retention in longitudinal studies have been examined, such as race and income (Boller et al. 2006; Wadsworth et al. 1992), there is limited research on how participants’ motivations for enrolling in a study and their study experiences impact retention.
Findings from a recent qualitative study suggest participant motivations for enrolling in a study can serve as a barrier if participants’ original motivations (e.g., need for information on rare diseases, money) for joining the study were not met. Alternatively, they can be a facilitator if motivations are adequately addressed or altruistic in nature (e.g., belief in research, volunteerism) (Odierna and Bero 2014). Few empirical studies have examined motivations for enrolling in a study or directly related these motivations to retention (Daniels et al. 2006; Lamvu et al. 2005).
The current research examines motivations for enrolling in a study and attitudes about study experiences and their influence on retention using data from the National Children’s Study (NCS) Vanguard Study. NCS was a series of pilot studies for a large-scale epidemiological cohort study of children and their mothers and fathers and originally planned as a 21 year longitudinal study.[1] NCS tested multiple recruitment strategies, data collection instruments, and protocols.
Methods
Design and Sample
Women who were age 18 or older[2] and pregnant/trying to become pregnant were recruited from 37 study locations across the country. NCS cohorts are distinguished by the methods used to recruit participants. The Initial Vanguard Centers (IVC) used in-person household enumeration. The Alternative Recruitment Strategies (ARS) included, direct outreach through advertisements to encourage self-referral (DO), household-based recruitment with enhanced outreach and engagement (EH), and recruitment through health care providers (PB). DO participants were subsequently divided into high (DO HI) and low (DO LI) intensity protocols. The DO LI protocol entailed fewer data collection events limited to phone interviews.
The current paper examines NCS cohort responses to the Participant Evaluation Questionnaire (PEQ). The PEQ was administered at the end of the participants’ first pregnancy data collection and included questions about reasons for enrolling in the NCS and study experiences. Participants in the IVC, EH, PB, and DO HI cohorts completed PEQ as a self-administered questionnaire. DO LI participants were administered PEQ through a telephone interview. Of the 4,554 women who completed the first pregnancy visit, 93 percent (n=4,216) completed the PEQ, with responses to individual items ranging from 94 percent (n=3,961) to 100 percent (n=4,216). There were no significant differences between PEQ respondents and nonrespondents (Table 1).
Measures
Reasons for Participation. Using a 3-point scale (not at all important, somewhat important, or very important), participants rated the importance of eight reasons for enrolling in the NCS. We examined the eight reasons separately and through factor analysis. For each of the reasons, we calculated univariate statistics and performed bivariate analysis to examine the association between retention and the reason. Factor analysis was conducted to reduce the number of items included in regression models. Findings indicated a one factor structure related to support for study participation.
General Experience. Women rated their general experience with the NCS using a 5-point scale (mostly negative, somewhat negative, neither positive or negative, somewhat positive, and mostly positive).
Interview Length. Participants rated interview length as too short, too long, or just about right.
Retention. Participants who had withdrawn from NCS or in tracing were considered inactive. All other participants were considered active and retained.
Statistical Analysis
Bivariate and multivariate analyses were conducted to examine associations between retention and PEQ measures, demographics, and recruitment strategy. Statistical analyses accounted for the clustered study design, with women sampled within geographic areas of study locations that followed each recruitment type. Chi-square tests were used to test associations between categorical variables. Logistic regression models were conducted to examine retention.
Results
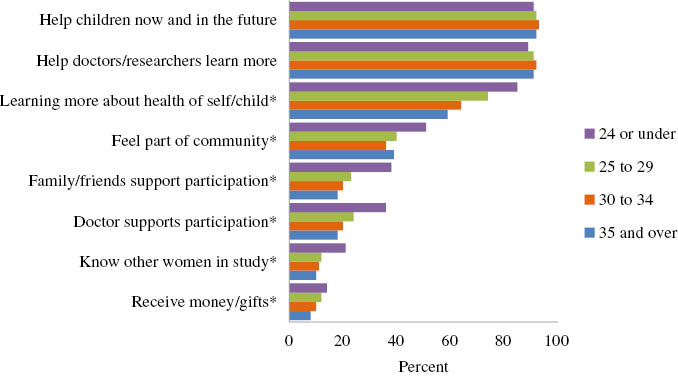
Reasons for Participation. Overall, helping children now and in the future and helping doctors/researchers learn more were rated as very important reasons for study participation. Receiving money/gifts and knowing other women in the study were least likely to be rated as very important (Table 2). However, within a given reason, there were some notable differences by demographic subgroups (Figures 1–3). For example, women who were younger, Hispanic or Black and had less education were more likely to rate knowing other women in the study as important. While receiving money/gifts was of relatively low importance overall, women with less than a high school education were three times as likely to report this as an important reason (18.8 percent) compared to women with a college degree (6.2 percent).

*Percent across categories are significantly different at p<0.05.
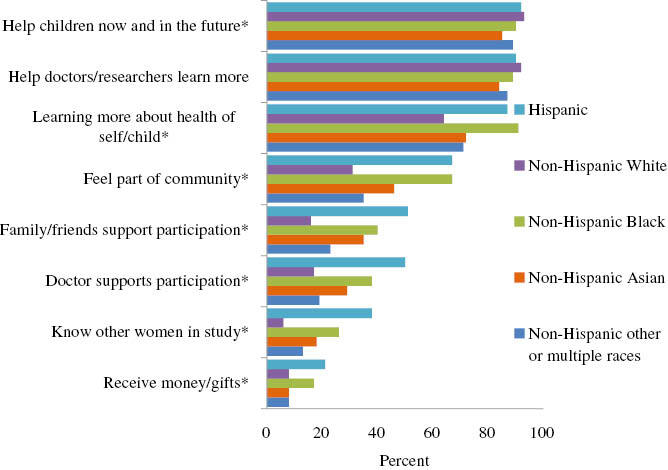
*Percent across categories are significantly different at p<0.05.

*Percent across categories are significantly different at p<0.05.
General Experience. Most women rated their experience in the NCS as mostly positive. Race/ethnicity and education were significantly associated with study experience (Table 3).
Factors Associated with Retention. Seventy-eight percent of women who completed the PEQ were retained in the NCS. Characteristics significantly associated with retention included being older, non-Hispanic White, married, more educated, and reporting a mostly positive study experience (Table 4) Five of the eight reasons for participation in the study had a negative significant association with retention (Table 5).
Logistic Regression. Age, factor score, and interview length were not significant in univariate models and excluded in subsequent models. Predictors in the final model were race/ethnicity, marital status, education, NCS study experience, and recruitment type. Characteristics associated with retention included being married (odds ratio [OR] 1.28; 95 percent confidence interval [CI] 1.07–1.52); having some college (OR 1.27; 95 percent CI 1.06–1.53); or having a college degree (OR 1.76; 95 percent CI 1.39–2.22) as compared to a high school degree or less, or being in the IVC or DO HI group compared with the DO LI group (OR 1.51; 95 percent CI 1.09–2.10 and OR 2.09; 95 percent CI 1.63–2.69, respectively). Women were less likely to be retained if they were Hispanic (OR 0.63; 95 percent CI 0.47–0.84), Asian (OR 0.62; 95 percent CI 0.44–0.87) or other/multiple races (OR 0.66; 95 percent CI 0.47–0.92), compared to White, non-Hispanic. Women with mostly positive NCS experience were more likely to be retained (OR 1.23; 95 percent CI 1.0001–1.52).
Discussion
While findings indicate the majority of NCS participants joined for altruistic reasons, many of the other reasons suggest a pattern of demographic differences. We found support-related reasons (doctor and family/friends support participation, feeling part of community, knowing other women in the study) and learning more about health of self/child were important among participants who were younger, Hispanic, not married, and less educated. Other researchers have found similar demographic patterns (Daniels et al. 2006; Lamvu et al. 2005).
Women who rated learning about health of self/child and support-related reasons as very important were significantly less likely to be retained in the NCS than those who did not rate these as important. Participants may be more likely to leave a study if they feel their primary reason for joining the study is not being met, which is consistent with findings from qualitative research conducted with former study participants (Odierna and Bero 2014). When controlling for demographics, reasons were not significant predictors for retention. Our findings indicated women who are White, married, and educated were more likely to be retained in the NCS. Similar patterns have been observed in other longitudinal studies (Patel, Doku, and Tennakoon 2003; Wadsworth et al. 1992). Personal motivations for joining research may not be the strongest factors influencing retention. We found positive study experience significantly positively associated with retention in the NCS even after controlling for demographics. Although participants in both DO cohorts volunteered for the study, DO LI had the lowest rates for positive study experience and retention and the DO HI had the highest rates. This suggests personal contact with study staff may positively contribute to retention.
The current study has limitations. Our analyses of PEQ responses followed the first pregnancy visit, and study experiences might be different after birth or many years. As with any self-reported data, there is a potential for bias. Our study contributes to the limited empirical literature on participant motivations and experiences in longitudinal research. The consistent pattern of demographic differences observed about motivations suggests future studies might benefit from tailored engagement strategies for demographic subgroups. Our findings also suggest in-person and more frequent data collection may be beneficial for retention. Longitudinal studies need to find a balance between overburdening participants and providing enough personal contact to retain participants.
Acknowledgment: This manuscript, a primary National Children’s Study (NCS) publication, was developed by a writing team assembled by the NCS Publications Committee for the purpose of timely sharing of centrally collected NCS data. The analysis was conducted as part of the NCS, supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and funded, through its appropriation, by the Office of the Director of the National Institutes of Health, under National Institute of Child Health and Human Development contract no. HHSN275201000013C.
The NCS is indebted to the many communities, families, and their health care providers whose participation made this study possible. The views expressed in this article are the responsibility of the authors and do not necessarily represent the position of the NCS, the National Institutes of Health, or the U.S. Department of Health and Human Services.
The NCS Vanguard Study was launched in January 2009 and continued until December 2014. Ultimately, the National Institutes of Health decided to cancel the study before full implementation.
Pregnant minors were included if permitted by state laws.